COVID-19 Vaccine Equity In Minnesota
From The Minnesota Department of Health
As the Minnesota Department of Health (MDH) has prioritized equity in its COVID-19 vaccine strategy, it is imperative to have metrics to both guide strategy and demonstrate accountability. Currently, demographic data (i.e., race, ethnicity, gender, and age) is included in the state’s public-facing COVID-19 vaccine dashboard. Persistent disparities in vaccination coverage by race and ethnicity necessitate strategic action toward health equity. To that end, congruent with the recommendations of scholars of vaccine ethics, MDH is addressing equity by using place-based strategies to allocate vaccine doses that incorporate a metric of community need (1)(2)(3)(4).
The Center for Disease Control and Prevention’s (CDC) Social Vulnerability Index (SVI) uses 15 indicators grouped into four themes that comprise an overall index measure. Communities with a high social vulnerability index generally have higher rates of poverty, crowded housing, racial/ethnic minorities, and lack of access to transportation when compared to communities with a low index (5). The index has been used by MDH and local public health agencies before and during the COVID-19 pandemic to calculate a weighted allocation of funding for pandemic/disaster preparedness and COVID-19 response efforts. The index is also recommended by the National Academies of Sciences, Engineering, and Medicine for prioritizing places in equitable vaccine distribution (6).
Additionally, counties with higher index scores have been shown to be at increased risk for COVID-19 outbreaks, particularly those with a higher percentage of racial and ethnic minority residents, high-density housing structures, and crowded housing units (7). Given the concerning rise of COVID-19 variant strands, focused allocation using this metric will: 1) help achieve more equitable distribution of COVID-19 vaccines, and 2) decrease the likelihood of future outbreaks among communities already hit the hardest.
Table 1. Minnesota COVID-19 burden by Social Vulnerability Index quartile, all ages, May 11, 2021
Using the ranked ZIP code areas of the state, MDH has determined the COVID-19 case rate, hospitalization, and death rates among Minnesotans from each quartile. It should be noted that because of how we have converted census tract data to ZIP codes, the percent of all Minnesotans in Quartile 1, or the “high” SVI quartile, using our methodology, is 29%. As of May 11, 2021, these 29% of Minnesotans have experienced 39% of all COVID-19 hospitalizations and 38% of deaths in Minnesota.
Table 2. Minnesota COVID-19 burden by Social Vulnerability Index quartile, under 17 years of age, May 11, 2021
Children under 17 years of age who live in “high” SVI ZIP codes in Minnesota have experienced 45% to date of all COVID-19 hospitalizations in this age group.
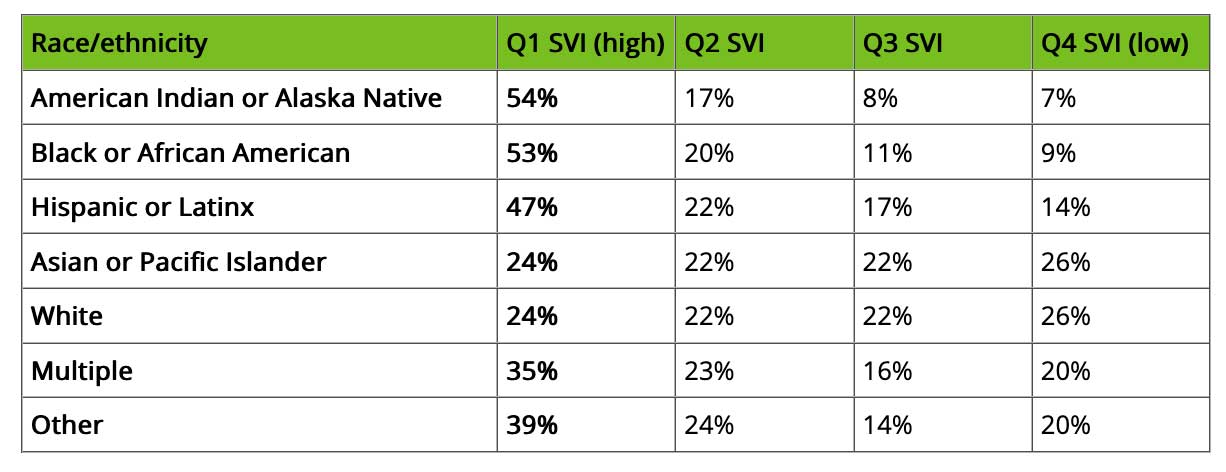
Table 3. Demographics of Social Vulnerability Index quartiles
MDH has also illustrated the demographic characteristics of Minnesotans who live in each quartile by race/ethnicity, limited English proficiency, disability status, and enrollment in a Minnesota health care program (MA/Medicaid or MinnesotaCare). These tables show the percentage of each category in each SVI quartile (e.g., 59% of Minnesotans with limited English proficiency live in Q1 SVI ZIP codes).
Equity Allocation Goal
To operationalize our equity metric, MDH has determined a specific allocation percentage prioritized for communities hit hardest by the COVID-19 pandemic using the Social Vulnerability Index ZIP code quartiles.
Our equity allocation goal for the state and our vaccinating partners is that 40% of all doses administered should be prioritized to the communities hit hardest by the COVID-19 pandemic.
MDH is tracking immunizations by vaccinator type and will be assessing the overall success of the state and our partners in eliminating the current gap for adults and preventing a gap among children as well as the performance of different vaccinators in reaching high SVI areas.
This equity metric and goals are one component of what is needed to truly operationalize equity in our COVID-19 vaccination efforts. Given what we know about the disparate impact COVID-19 has had on communities in Minnesota, the structural and societal barriers many children and families face in accessing even routine care and the disparities we have already seen in COVID-19 vaccine rates for adults, it is critical that pediatric providers take steps not only to mitigate further inequities in access, but to continue to build a more just and community-driven approach to health in response to the COVID-19 pandemic.
References
- Persad, G., et al. (2020). Fairly Prioritizing Groups for Access to COVID-19 Vaccines. JAMA 324(16): 1601.
- Schmidt, H., et al. (2020). Is It Lawful and Ethical to Prioritize Racial Minorities for COVID-19 Vaccines? JAMA 324(20): 2023.
- Schmidt, H., et al. (2020). Covid-19: how to prioritize worse-off populations in allocating safe and effective vaccines. BMJ: m3795.
- Shen, A. K., et al. (2021). Ensuring Equitable Access To COVID-19 Vaccines In The US: Current System Challenges And Opportunities. Health Affairs 40(1): 62-69.
- Centers for Disease Control and Prevention/ Agency for Toxic Substances and Disease Registry/ Geospatial Research, Analysis, and Services Program. CDC Social Vulnerability Index, 2018 Database, Minnesota. https://www.atsdr.cdc.gov/placeandhealth/svi/data_documentation_download.html. Accessed on March 31, 2021.
- National Academies of Sciences, Engineering, and Medicine. 2020. Framework for Equitable Allocation of COVID-19 Vaccine. Washington, DC: The National Academies Press. https://doi.org/10.17226/25917.
- Association between social vulnerability and a COUNTY’S risk for becoming A COVID-19 hotspot – United STATES, June 1–JULY 25, 2020. (2020, October 22). Retrieved February 20, 2021, from https://www.cdc.gov/mmwr/volumes/69/wr/mm6942a3.htm.
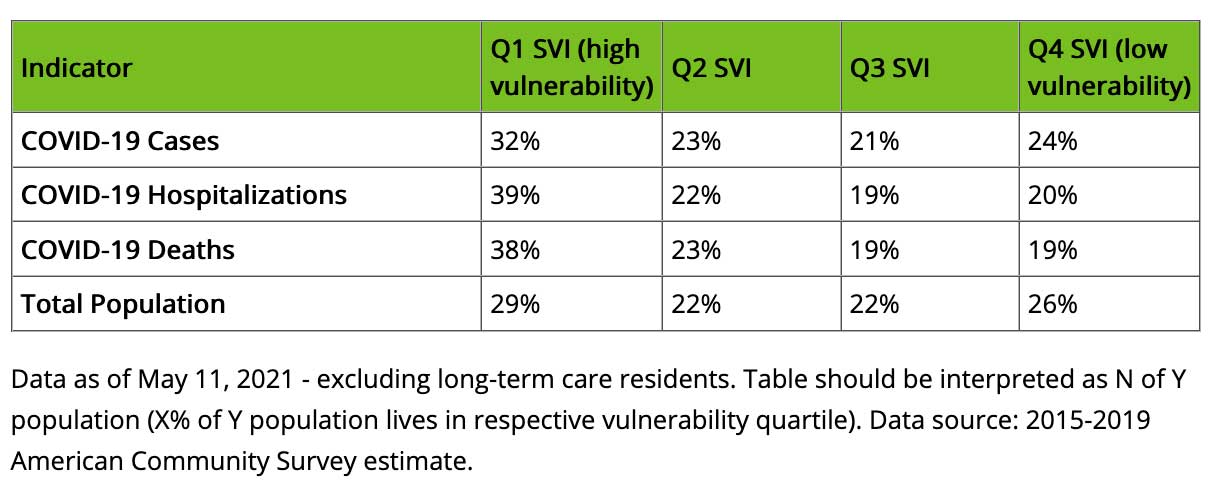
Table 1. Minnesota COVID-19 burden by Social Vulnerability Index quartile, all ages, May 11, 2021